郭某某,男,65岁 Mr.Guo,male,65 years old 一、病例特点 General Information 病史 现病史:患者于入院前4小时突发右眼胀痛,伴头痛。来我院门诊就诊发现眼压高,药物控制不佳。 眼病史:左眼抗青光眼术后10余年。既往史:既往体健。 个人史、家族史均无异常。 Medical history: Presenthistory : The patient had a sudden eye pain in his right eye,accompanied with headache for 4 hours .The IOP was above normal anduncontrolled by drugs . Past history : Trabeculectomy was performed in his left eye 10 yrs ago . Personal history, family history showed no abnormality 眼部检查: 右眼:VOD0.5,IOP55mmHg,结膜充血,角膜肿,旁中央可见粘连性角膜白斑,前房浅,中轴1.5CT,周边,1/4CT,瞳孔直径2mm,瞳孔缘虹膜后粘,晶状体混浊,眼底窥不清。(图1) 左眼:VOS0.4,IOP17mmHg, 结膜滤过扁平,角膜透明,前房中轴2CT,周边,1/3CT,瞳孔直径5mm,晶状体混浊,眼底C/D0.8。Ocular examination : Right eye : VOD0.5 IOP55mmHg, conjunctival congestion, corneal edema, paracentral adherent corneal leukoma, anterior chamber was shallow, 1.5CT in the center, 1/4CT peripherily. The pupil diameter was 2mm. with partial posterior synechia. The lens was opaque, and the funds was unreachable.(fig 1) Left eye: VOS0.4 IOP17mmHg,bleb flattened, cornea clear, anterior chamber was shallow with 2CT in the center, 1/3CT peripherily, The pupil diameter was 5mm, the lens cortex has mediate opacity, and C/D showed 0.8 . 二、辅助检查 Auxiliary examination B超:左眼玻璃体混浊(图2)B scan: vitreous opacity in left eye. (fig 2) 三、初步诊断 Impression 右眼急性闭角型青光眼发作期合并粘连性小瞳孔双眼玻璃体混浊双眼老年性白内障 左眼抗青光眼术后 右眼粘连性角膜白斑 Acute angle-closure glaucoma accompanied with adhesive small pupil OD Vitreous opacities OU Age-related cataract OU Post trabeculectomy OSAdhaerent Corneal Leukoma OD 四、药物治疗 Medication 入院第1天:甘露醇250ml静脉点滴 bid,尼目克司25mg Bid,派立明OS TID, 阿法根 OS tid 降眼压。 入院第2天:VOD手动/眼前,角膜水肿加重,考虑不除外瞳孔阻滞,予YAG虹膜激光周边切除术,眼压未降,IOP57 mmHg。入院第3天:甘露醇250ml后,行左眼白内障超声乳化+人工晶状体植入术+复合小梁切除术,手术顺利。 术后第1天:VOD手动/眼前,角膜水肿明显,前房纤维素样渗出,滤过弥散,人工晶状体位正,IOP15mmHg。常规抗炎点眼治疗,隔日球旁注射地塞米松5mg。术后10天:VOD手动/眼前,角膜水肿减轻,前房渗出吸收,眼压正常,发现玻璃体灰白色混浊,后部窥不入。 行B超检查:右眼玻璃体弥漫点状低回声,膜状中强回声。(图3) First day: The patient was given 250ml mannitol twice a day, Wethazolamide 25mg twice a day, Azopt OS Tid, Alphegan OS TID to controll his intraocular pressure. Second day: The patient had a sudden decreasing of visual acuity. VOD HM, corneal edema more severely, It was considered pupillary block, and then the laser peripheral iridectomy was performed, but is unhelpful to control IOP which is still was 57 mmHg. Third day: The patient was given 250ml mannitol, and then underwent phacoemulsification, intraocular lens implantation combined with trabeculectomysmoothly. First day after operation: VOD HM, corneal edema, fibril exudation in the anterior chamber, filtration bleb diffussed, IOP was 15mmHg .Anti-inflammatory eye drops was given, and 5mg dexamethasone peribulbal injection every other day. 10th day after operation: VOD HM, corneal edema was relieved, exudation absorbed, the intraocular pressure was normal, but the vitreous cavity was found opacity. B scan: There was diffuse hypoechoic spots, lumps, and strong echo membrane in the vitreous cavity. (fig 3) 五、查房记录 Discussion 刘增业主任医师 患者手术顺利,眼压稳定,视力不能恢复主要因为玻璃体混浊所致;分析原因1)感染性眼内炎;2)无菌性炎症;3)玻璃体积血。患者玻璃体混浊为灰白色,前节反应不重,不除外弱菌感染眼内炎,例如表皮葡萄球菌感染性眼内炎。 术后第11天:予万古霉素10mg/ml局部点眼Q2h,隔日予万古霉素50mg/ml,地塞米松2.5mg球旁注射,共14天,未见明显缓解。隔日复查B超检查:右眼玻璃体弥漫点状中低回声,膜状中强回声。(图4) 术后25天:VOD手动/眼前,玻璃体混浊,B超检查:右眼玻璃体弥漫点状中低回声,膜状中强回声。(图5) 术后1月:行右眼后部玻璃体切割术。术中玻璃体及前房水培养未查见病原体,仅见网膜点状出血,考虑玻璃体混浊性质为玻璃体积血,术后视力恢复为0.5,眼压稳定,网膜在位。(图6、7) 总结 高眼压下青白联合手术,增加术中及术后出血风险,同时考虑存在恶性青光眼因素。术前患者突发视物不清,应及时复查彩超,明确病因;术后玻璃体混浊原因不明,选择合适时机行玻璃体切割手术明确病因,以利患者恢复视力。 Dr. Liu Zeng-Ye: visual acuity cannot be recovered, most likely due to vitreous opacities which is relative to ; 1) infectious endophthalmitis; 2) the aseptic inflammation; 3) vitreous hemorrhage. Since the vitreous opacity was gray, yet the anterior segment reaction was not heavy,the low virulence bacterial induced endophthalmitis can not be excluded such as Staphylococcus epidermidis. 11th day after operation:Treated with vancomycin (10mg/ml)OD Q2h, then vancomycin (50mg/ml) and 2.5mg dexamethasone peribulbal injection every other day. B scan was examined every other day. (fig 4) 25th day after operation: VOD HM, vitreous opacity. B scan: There was diffuse hypoechoic spots, lumps, and strong echo membrane in the vitreous cavity. (fig 5) 30th day after operation: the right eye underwent vitrectomy. During the operation,the vitreous and aqueous was extracted and sent to stain and culture,but no pathogens was found. The retina was found spot hemorrhage, which may contribute to the vitreous opacity. After vitrectomy, visual acuity was 0.5, intraocular pressure was nomal, and retina attached. (fig 6、7) Summary: It will increase the risk of bleeding when performing the combined surgery of glaucoma and cataract under high IOP. The malignant glaucoma must be alerted in this condition. Before operation, when sudden vision blurring happened, the B scan should be done to find the abnormalities.If not confirmed, the vitrectomy should be considered to restore vision as necessary as we can.. 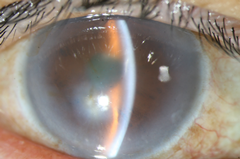
图1 Fig1 入院第1天 First day
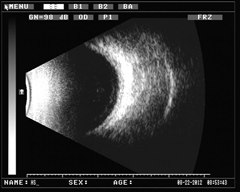
图2 Fig2 入院第1天 First day
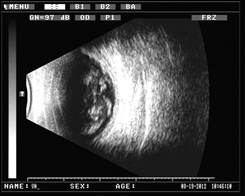
图3 Fig3 前三联术后第10天 P/s 10d(phaco+IOL+trabeculectomy)
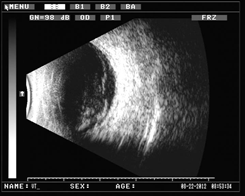
图4 Fig4 前三联术后第11天 P/s 11d(phaco+IOL+trabeculectomy)

图5 Fig5 前三联术后第25天 P/s 25d(phaco+IOL+trabeculectomy)

图6 Fig6 玻璃体切割术后 P/s TPPV

图7 Fig7 玻璃体切割术后 P/s TPPV |